
Thyroid
Clinical history:
46 year old woman with documented primary hyperparathyroidism. She has complaints of joint pain and fatigue. A DEXA scan confirmed advanced osteoporosis. Ultrasound was requested prior to parathyroidectomy.
Laboratory:
Serum calcium of 10.2 mg/dL
PTH of 124 pg/mL





Results:
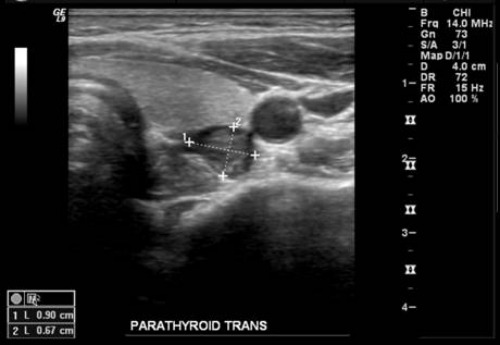
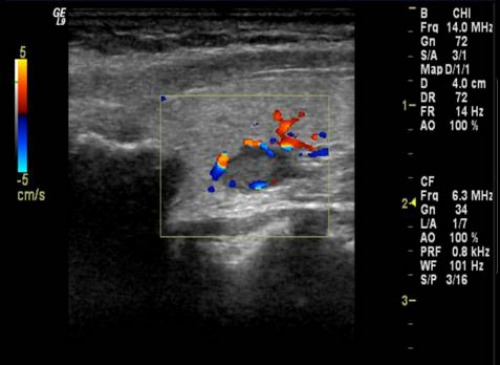
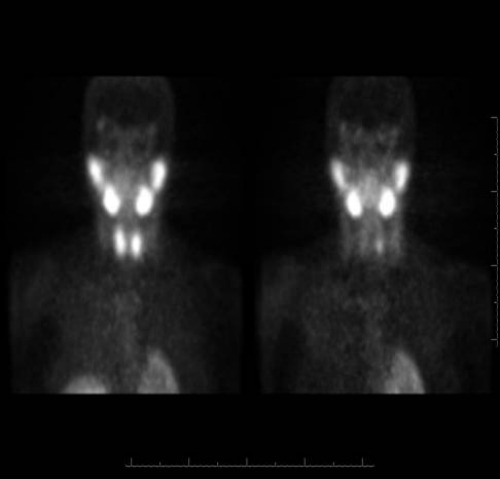
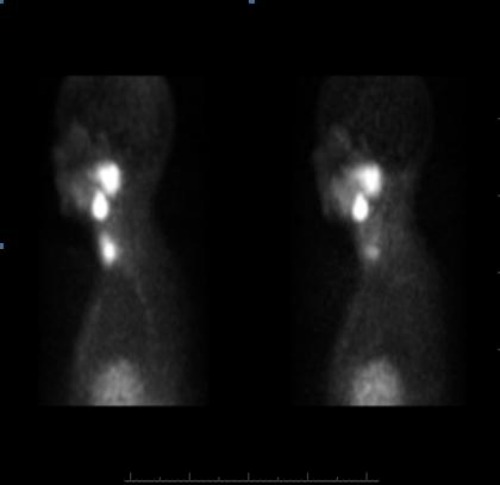
These Sonographic and Tc99m Sestamibi images were consistent with findings of a descended superior parathyroid adenoma which was proven at exploration.
Questions:
Which of the following are sonographic characteristics of parathyroid adenomas? (More than one may be correct)
- Solid
- Hypoechoic
- Oval Shape
- Hypervascular (Variable)
- Posterior to Thyroid
- Medial to Carotid
Where are common locations of ectopic parathyroid adenomas? (More than one may be correct)
- Low Neck
- Mediastinum
- Retrotracheal/Retroesophageal
- Carotid Sheath
- Intrathyroid
True or false: Normal parathyroid glands are usually seen on sonography?
Answers:
Which of the following are sonographic characteristics of parathyroid adenomas? (More than one may be correct)
All of the above are correct. Please see discussion for details.
Where are common locations of ectopic parathyroid adenomas? (More than one may be correct)
All of the above are correct. Please see discussion for details.
True or false: Normal parathyroid glands are usually seen on sonography?
False. Please see discussion for details.
Most individuals have 4 parathyroid glands: 2 superior and 2 inferior. The superior glands are usually posterior to the upper or mid pole of the thyroid gland. The inferior glands have a variable location but are usually inferoposterior to the thyroid. Normal parathyroid glands are not reliably seen on sonography and measure approximately 1x3x5 mm.
University of Pittsburgh Medical Center
Department of Radiology
References:
- Kwak, JY, et al. Findings of Extrathyroid Lesions Encountered With Thyroid Sonography. J Ultrasound Med. 2007; 26: 1747–1759.
- Reeder, SB, et al. Sonography in Primary Hyperparathyroidism. J Ultrasound Med. 2002; 21: 539-552.
- Johnson, NA, et al. Parathyroid Imaging: Technique and Role in the Preoperative Evaluation of Primary Hyperparathyroidism. AJR. 2007; 188: 1706-1715.
- Tublin, ME, et al. Localization of Parathyroid Adenomas by Sonography and Technetium Tc 99m Sestamibi Single-Photon Emission Computed Tomography Before Minimally Invasive Parathyroidectomy. J Ultrasound Med. 2009; 28: 183-190.
- Middleton, WD, et al. Ultrasound: The Requisites. 2004; 253-257.